Alveolar Ridge Preservation & Bone Regeneration Procedures
When tooth loss occurs, the underlying bone naturally begins to shrink. This bone loss compromises the success of dental implants, alters facial structure, and affects adjacent teeth. The advanced bone regeneration procedures, including alveolar ridge preservation, guided bone regeneration (GBR), and guided tissue regeneration (GTR), offer comprehensive solutions for both extraction sites and around existing teeth and implants. These techniques can preserve existing bone and/or actively regenerate lost tissue, whether for preparing for future implants, treating bone loss around natural teeth, or addressing complications around existing implants. By regenerative therapy, patients maintain their facial support, preserve implant candidacy, and create healthy, stable foundations that support long-term oral health success.
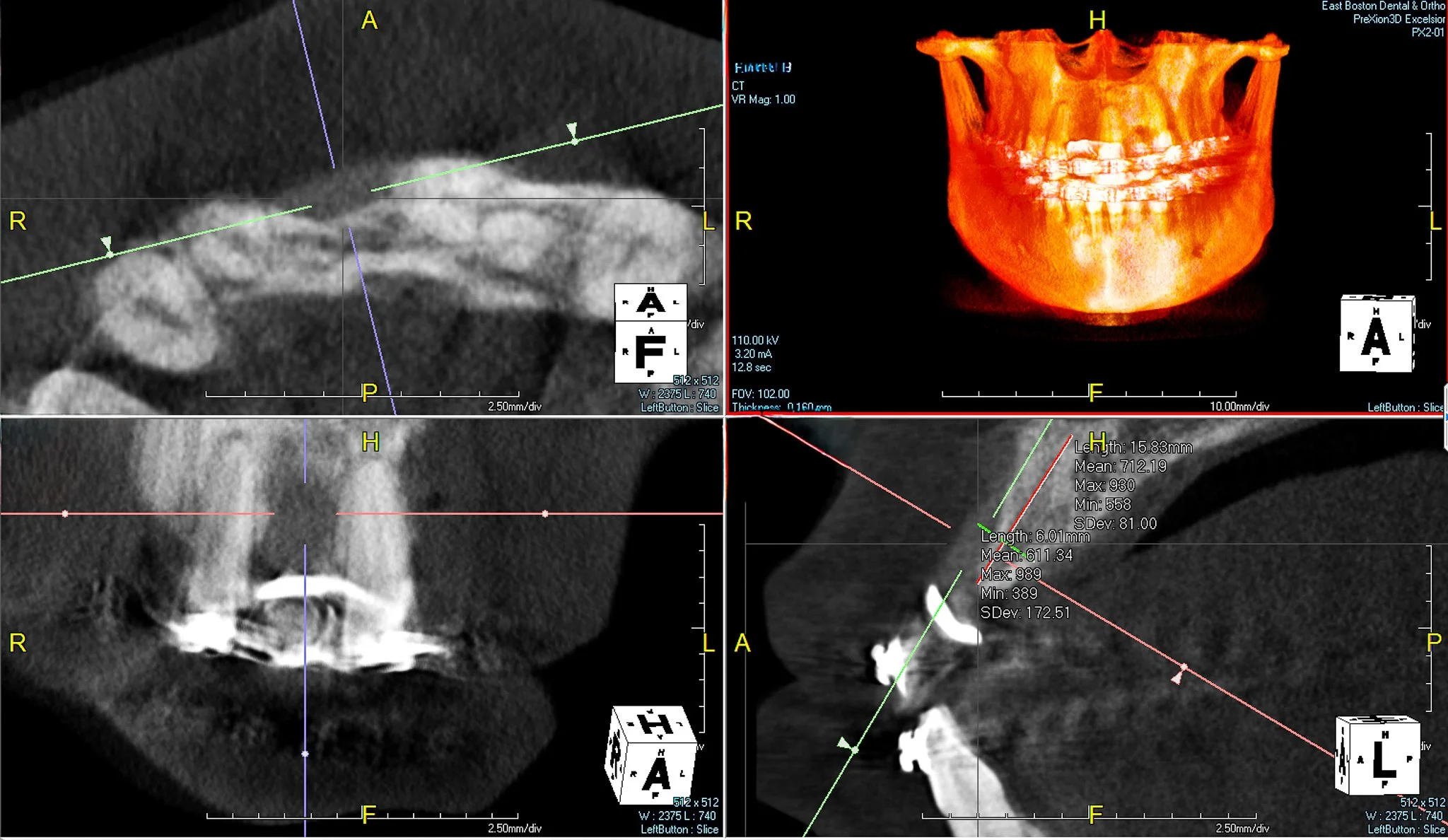
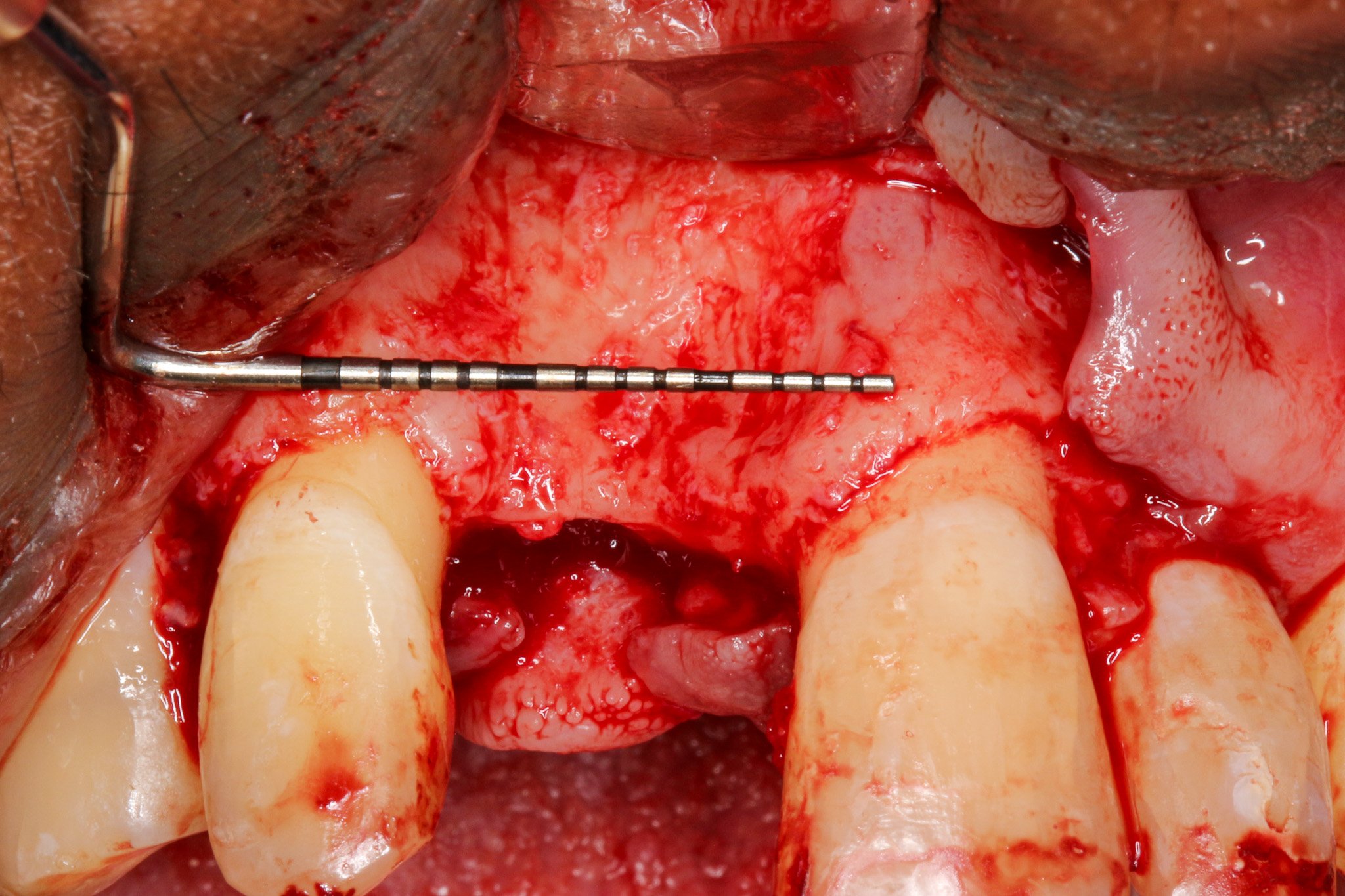
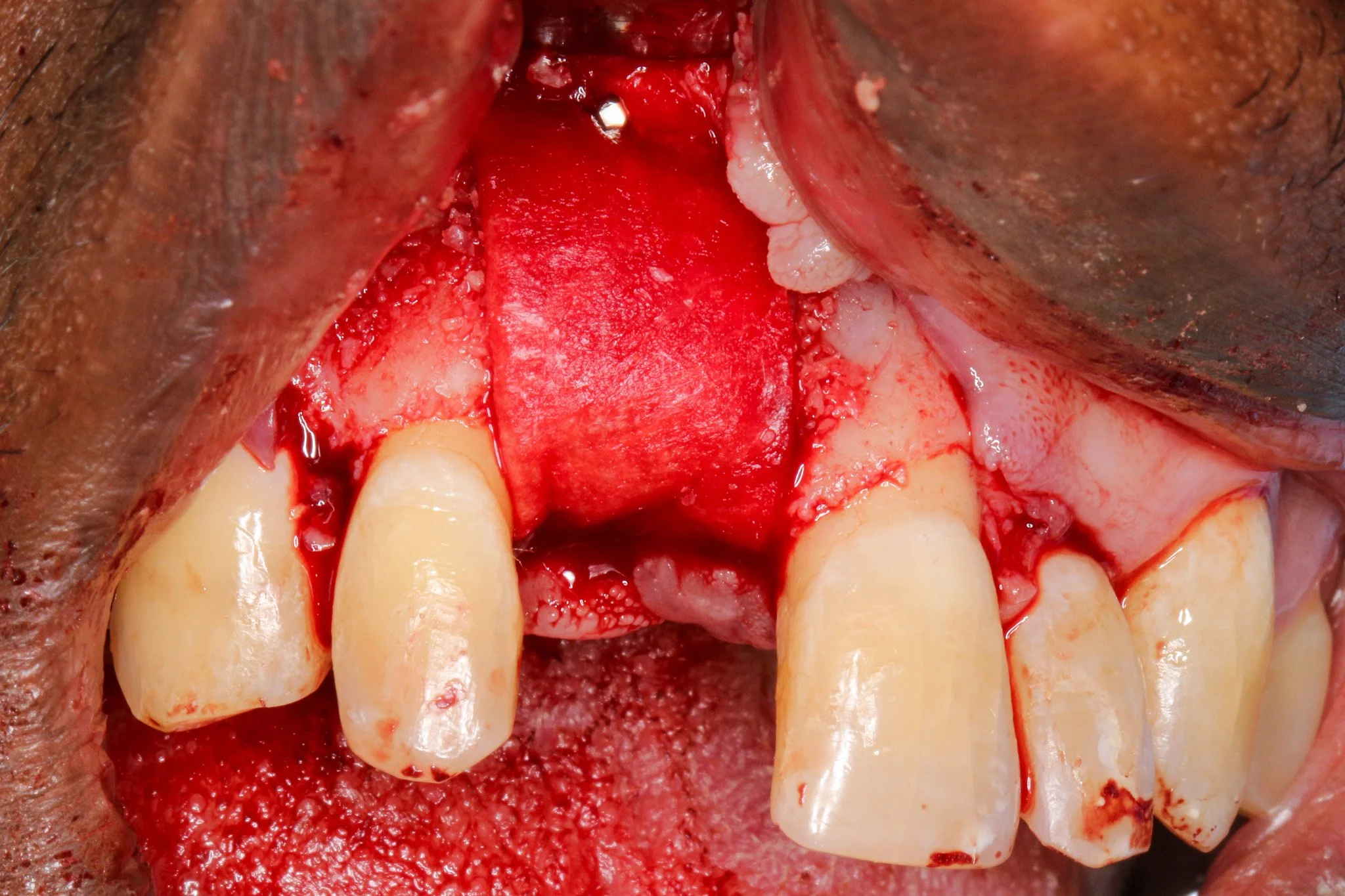
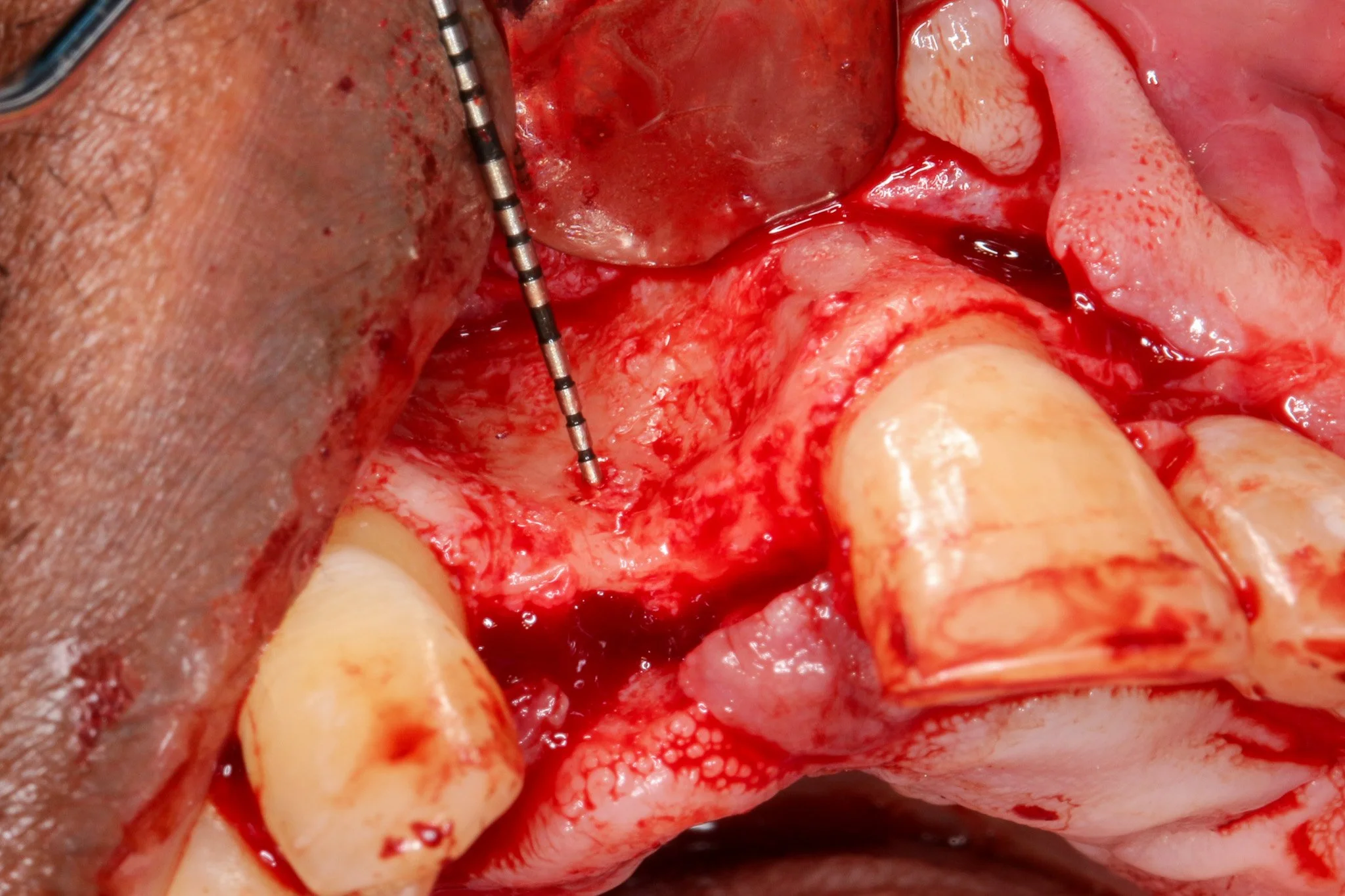
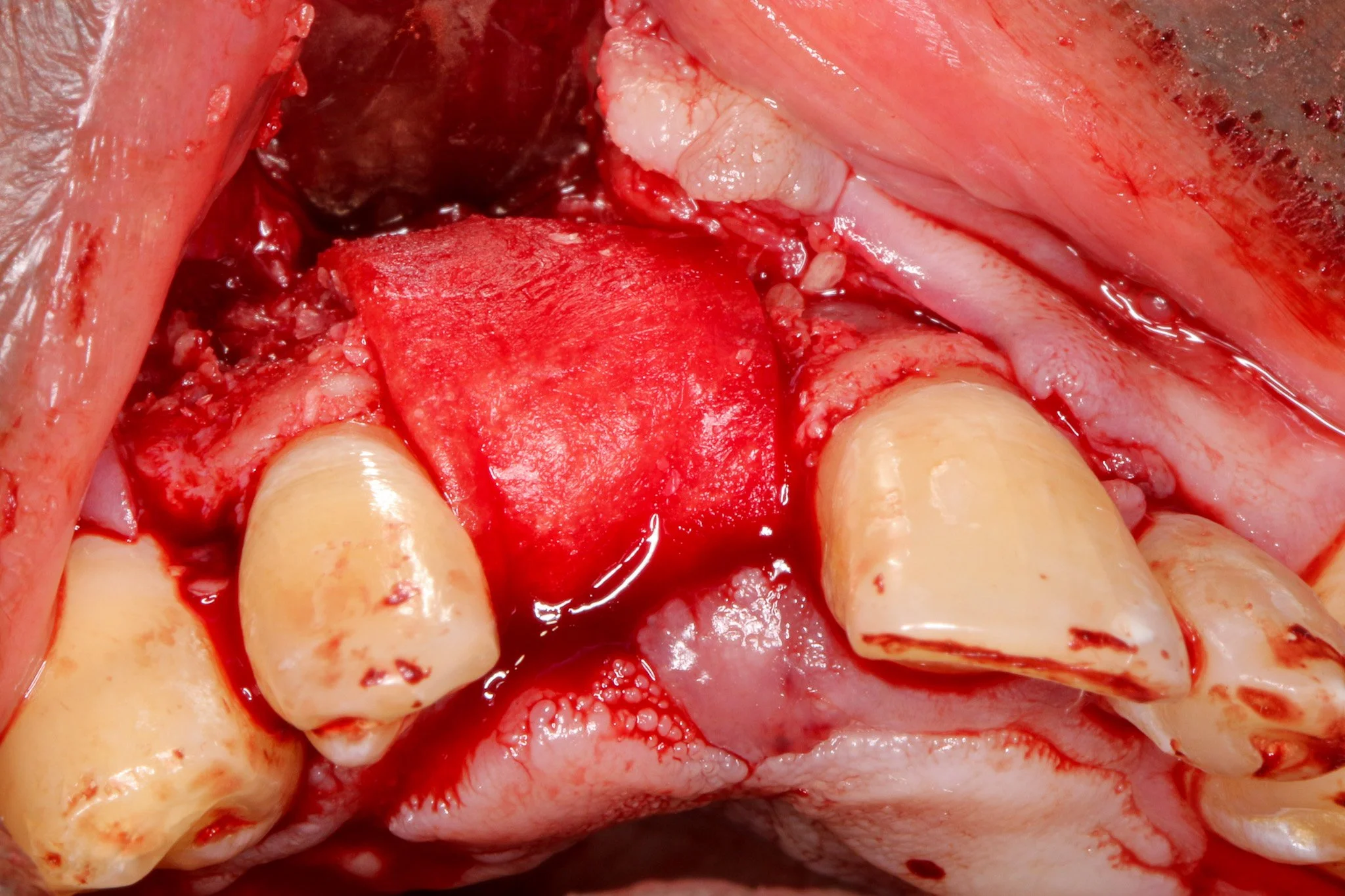
4 to 5 mm buccal bone dehiscence with concave morphology.
Thorough scaling and root planing of adjacent teeth was performed to minimize bacterial load as periodontal health is critical for GBR success; inflammatory conditions can compromise graft integration and membrane barrier function (Simion et al., 1994)
A 33 year-old male patient has been missing #8 for more than a decade due to physical trauma in the area. The patient had given treatment options of a bridge and a dental implant. After a thorough discussion among the patient, the restorative dentist, and me, we came to the conclusion that a dental implant will be a more optimal and definitive treatment for the patient.
As you can see, there is a buccal-palatal concavity from the axial view on #8. Thus, GBR was planned for horizontal ridge augmentation to address a significant buccal bone dehiscence.
Periosteal releasing incision was executed to achieve tennsion-free, passive primary closure. Wang and colleagues 2001 demonstrated that passive flap closure significantly reduces membrane exposure rates and enhances bone regeneration outcomes. It is important to preserve blood supply to soft tissue while allowing adequat flap advancement when periosteal releasing incision is made.A double-layer resorbable membrane technique was employed with tacking srew fixation to ensure graft stability and space maintenance. The use of resorbable membranes has been extensively validated in the literature, with systematic reviews by Rocchietta et al. (2008) confirming comparable outcomes to non-resorbable membranes while eliminating the need for 2nd stage surgery. Urban et al. (2009), the dual-membrane approach provides enhanced barrier function and structural support.

An ePTFE (polytetrafluoroethylene) suture was selected for its superior handling characteristics, minimal tissue reactivity, and reduced bacterial adhesion compared to conventional suture materials (Lilly et al., 2016). A double-layering suture technique combining horizontal mattress sutures with single interrupted sutures was implemented. Horizontal mattress sutures effectively evert wound edges and distribute tension away from the incision line (Burkhardt et al., 2008). Interrupted sutures ensure intimate tissue contact and optimal healing, which protects the underlying graft and membrane from bacterial infiltration. This sophisticated suturing approach has been shown to significantly reduce early wound dehiscence rates, particularly critical in GBR procedures where membrane exposure can compromise regenerative outcomes (Zucchelli et al., 2013).This systematic approach addresses the multifactorial nature of GBR success, including infection control, space maintenance, membrane stability, and primary soft tissue closure.The excellent healing observed in this case exemplifies the importance of meticulous surgical execution and adherence to biological principles. Following appropriate healing time, this regenerated ridge will provide adequate bone volume for ideal three-dimensional implant placement with enhanced long-term aesthetic and functional outcomes.